

The 4 Kinds of Universal Healthcare
Single-payer isn't the only option

You’ve probably heard that the United States is the only high-income country in the world that doesn’t have Universal Healthcare. That’s true.
In all advanced nations other than the United States, the government makes an organized effort to control costs, achieve universal access, and promote quality.
They go about achieving this in different ways. There are broadly four different approaches: [1] Socialized Medicine, [2] Single Payer, [3] Managed Competition, and [4] Two Tier.
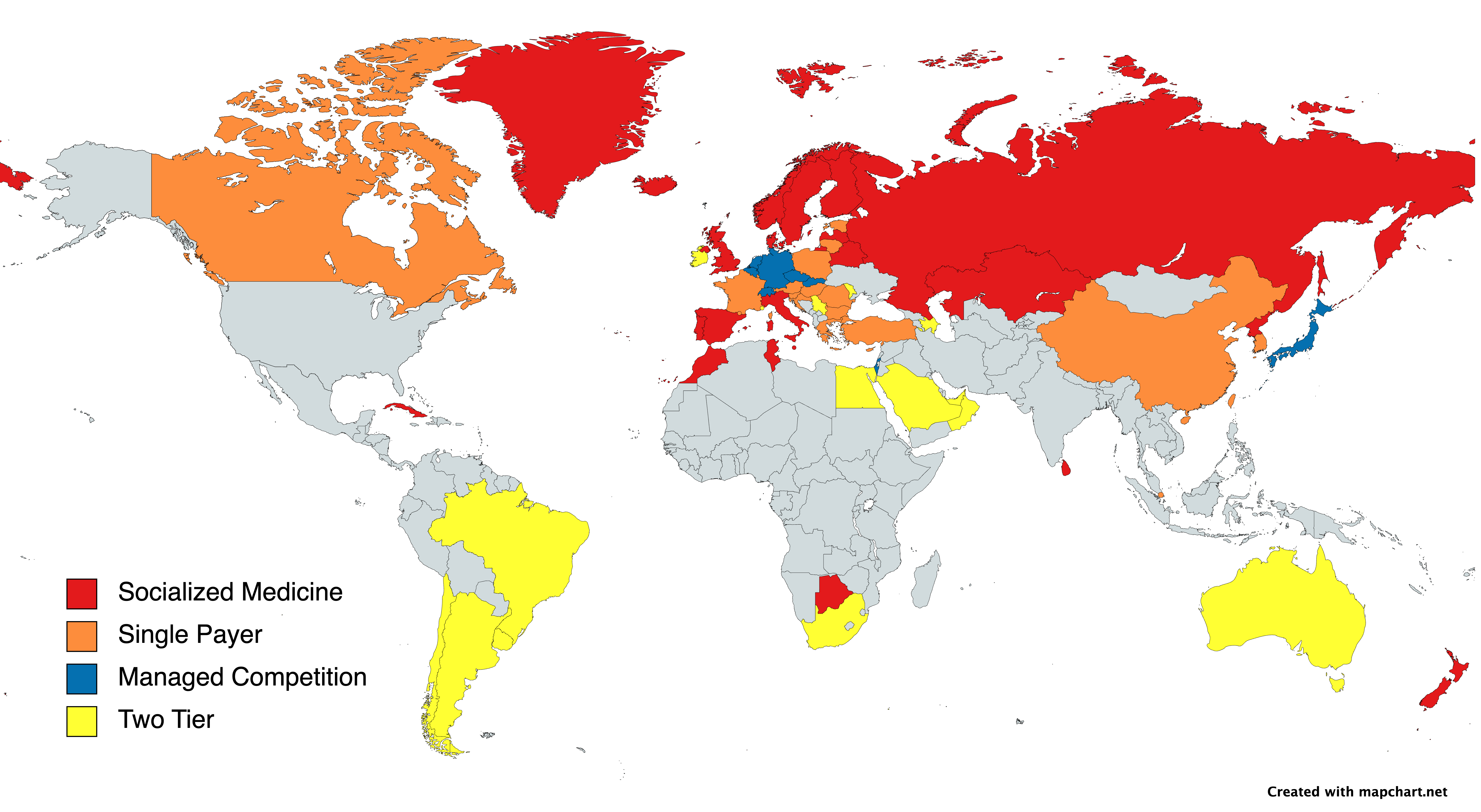
[1] Socialized Medicine
DESCRIPTION
Insurance: Public
Providers: Public / Mixed
In countries that have socialized medicine, both financing and delivery of healthcare are organized by the government. All citizens are guaranteed access to care at low or no cost, with the system funded by taxes.
Public hospitals receive a pre-determined, fixed annual budget rather than payment by insurance for services provided. This practice is often referred to as “global budgeting.”
In the purest forms of socialized medicine, like Cuba, clinics for primary and specialty care are also publicly run. Yet, in other countries that otherwise should be considered socialized medicine, independent primary care and specialist clinics exist and are incorporated within the public system.
Countries with socialized medicine vary in what level of government predominantly manages the system. In Scandinavia, healthcare provision is organized by municipal and regional governments. Meanwhile, in the United Kingdom, the central government plays a much more pronounced role.
Duplicative insurance, i.e., insurance that provides coverage for the same thing the public system provides coverage for, is often restricted. Private supplemental coverage for things not covered by the public system, on the other hand, is usually permitted.

[2] Single Payer
DESCRIPTION
Insurance: Public
Providers: Private / Mixed
Single-payer systems feature insurance provided by the government, with usually a mixture of public and private providers. Funding for the insurance comes from taxes or employer and employee contributions. However, in a select few places, like the Canadian Provinces of Ontario and British Columbia, a small premium is charged.
The level of deductibles, copays, and coinsurance depends on the country. In Taiwan, copays and coinsurance are used liberally to cut down on use. In Hungary, there is little to no cost sharing, and the state opts to use care rationing when demand for care outstrips supply.
Not all countries I have classified as single-payer technically have a *single* payer. In some countries, like Austria, there are technically multiple insurance funds that people are assigned to based on variables like region, industry, and employment status. These funds do not compete with one another and are all managed by the state. They also provide the same coverage and operate based on the same reimbursement scheme. For these reasons, there is no practical reason to classify these systems as anything other than single-payer because they operate exactly the same way.
Similar to socialized medicine, duplicative insurance is often prohibited in countries with single-payer insurance, but supplemental and complementary insurance coverage is permitted and relatively common.

[3] Managed Competition
DESCRIPTION
Insurance: Private
Providers: Private / Mixed
The most market-oriented of all approaches to universal healthcare managed competition systems rely on a regulated competitive private insurance marketplace. Plans are required to cover a standard government-mandated package of services. Cost sharing is regulated if not completely standardized across plans.
Discrimination against those with preexisting conditions is strictly prohibited. Insurers are required to charge the same price to everyone (except age price discrimination, which is permitted in some places); this practice is referred to as “community rating.” Guaranteed issuance is enforced, meaning insurance companies are never permitted to reject someone who wishes to enroll in their plan.
Because insurers are no longer allowed to charge riskier patients more, a new problem is introduced. Some insurers have, on average, more expensive patients to cover than others, leading them to perform worse through no fault of their own.
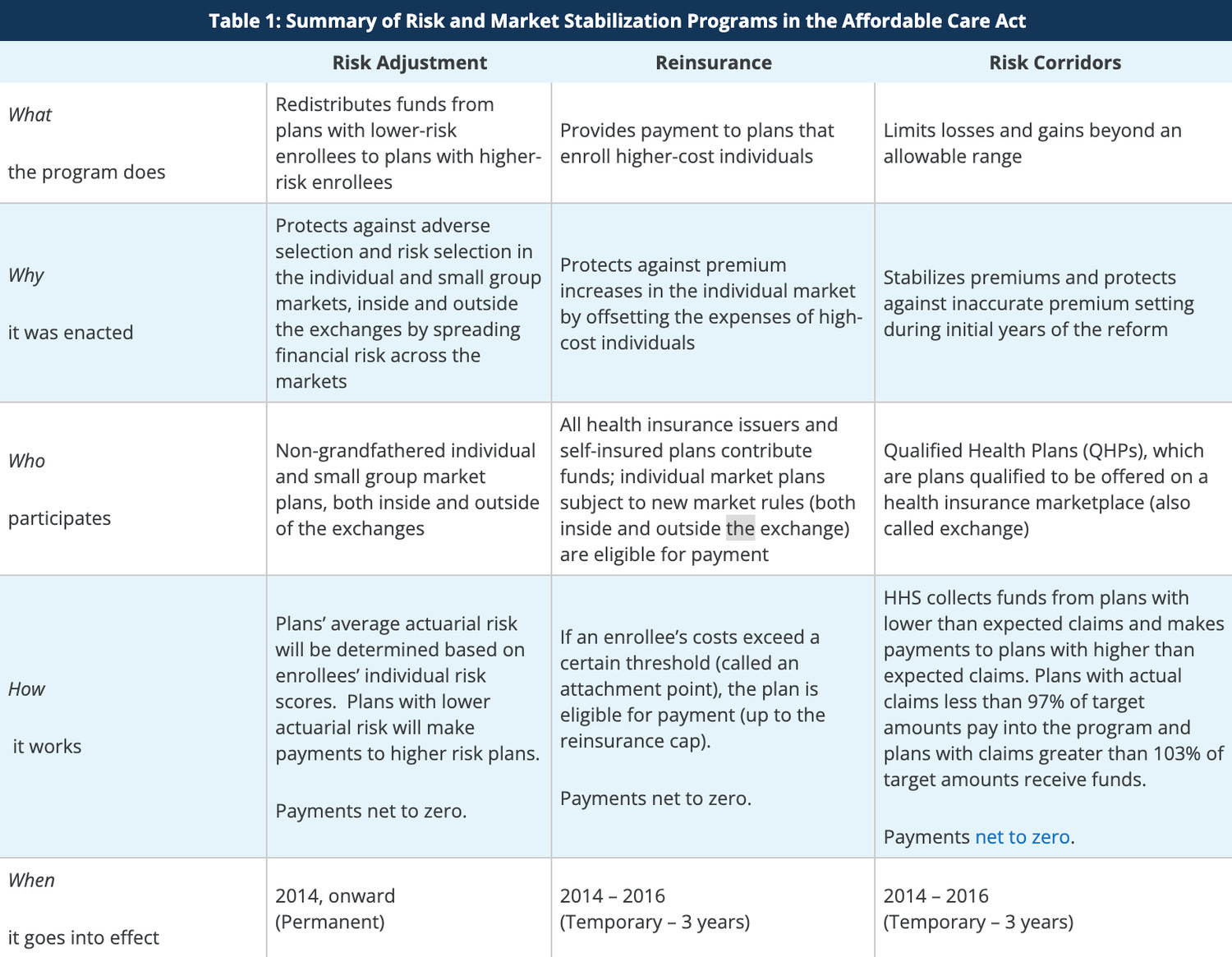
To correct this problem, the government establishes risk rebalancing procedures. The most basic of these that all systems employ is called “risk adjustment.” Under risk adjustment, plans that have on-average, healthier patients are charged, and plans that have on-average, less healthy patients are subsidized.
Determinations of people’s health are made using an algorithm that takes into account people’s age, gender, and comorbidities, amongst other variables.
Shopping for insurance is made easier by all of them being available on a centralized marketplace that makes information on the differences between the plans easy to digest. Plans compete on what additional coverage they provide and, in some countries, their premiums and networks.
Cost sharing is common, and insurance plans are funded either by employer and employee contributions or traditional premiums with subsidies provided to those with lower incomes. Some countries have public options, which compete with private options in the insurance market. This is what happens in present-day Slovakia.
Providers consist of a mixture of public firms, for-profits, and non-profits. In some countries, reimbursement rates for providers are centrally negotiated, a process referred to as all-payer rate setting. In these systems, insurance networks do not exist.
In other countries, reimbursement rates are decentrally negotiated, and insurance networks remain.

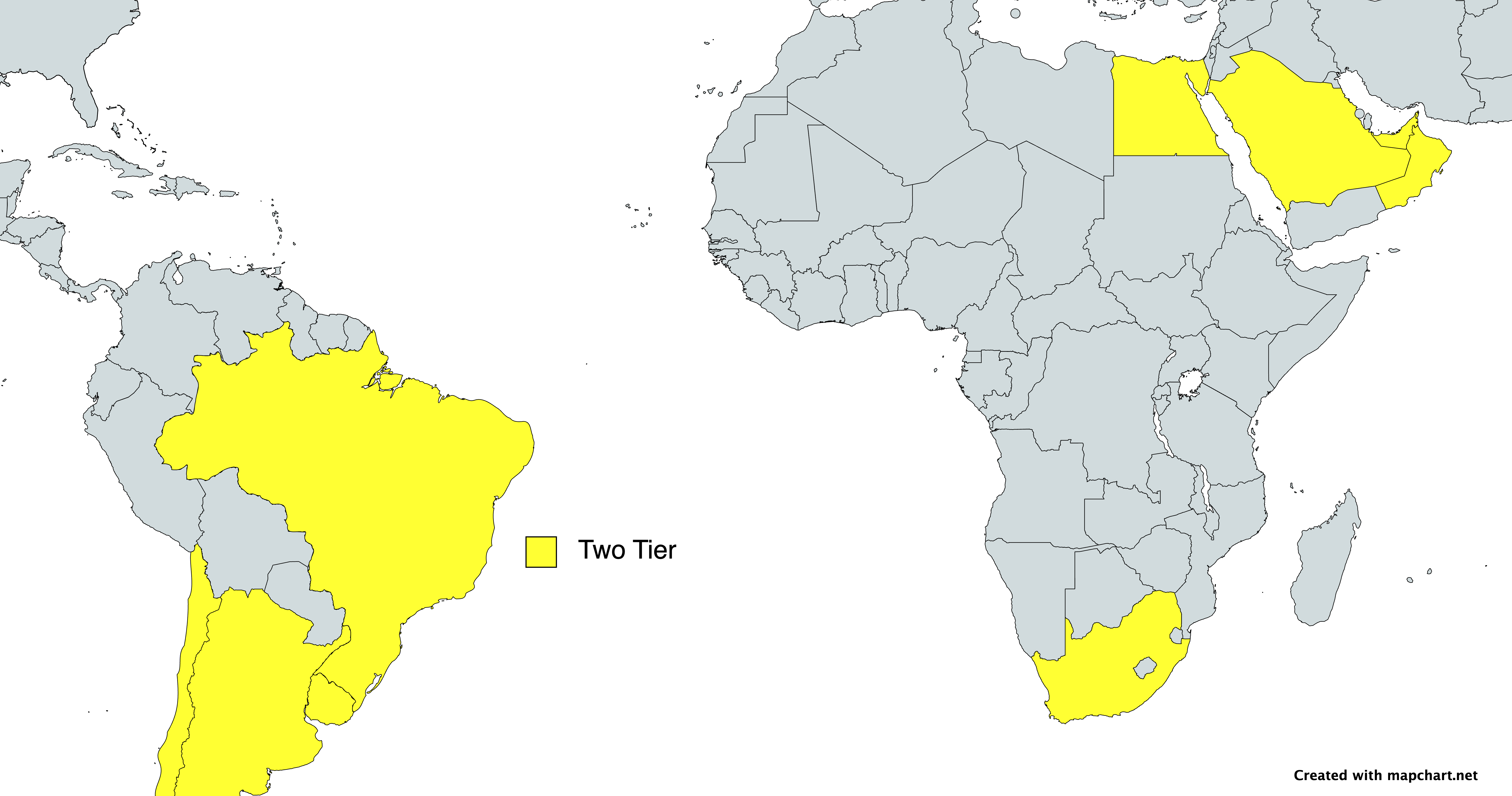
[4] Two Tier
DESCRIPTION
Insurance: Mixed
Providers: Mixed
Two tier healthcare systems are those that feature both an expansive public system and a separate expansive private system. The public system is most commonly a form of socialized medicine, although occasionally, it can be closer to a single-payer or managed competition model. The private system is lightly regulated, with private insurers and providers mostly determining their own policies as they would in an unobstructed market.
To differing degrees, many countries that have socialized medicine, single payer, or managed competition have some extent of an additional private system. For instance, in Germany, 11% of the population receives their health insurance through one of the independent private insurers rather than a regulated sickness fund.
The delineation between non two tier systems and two tier systems is not always the clearest, but for our purposes, I have come up with two criteria:
The private system must be a comprehensive alternative to the public system. A private system that just consists of supplementary services to the public system or offers a replacement for some but not all of the public system's functions is insufficient.
The size and scope of the private system must be large enough to constitute a genuine option for the majority of the population.
Australia represents the quintessential example of a two tier system.
All Aussies are entitled to coverage under the national health insurance program Medicare. Medicare guarantees access to public primary, specialty, and hospital care, with very low levels of cost sharing.
But in addition to Medicare, as of 2023, 45% of Australians have non-supplemental private health insurance. This private insurance provides them access to an array of health services and commodities not available in the public system.
Two tier systems are often the result of political compromises. In Australia, the tug of war between the Labor Party and the Liberal Party has kept both the public system and the private system alive, with neither overtaking the other.
Both parties seem to have come to terms with its continued existence but with disagreements about what the proper role of each part is.
Labor thinks the public system should be more robust, and private insurance should remain mostly as a thing that only high-income Aussies feel the need to opt for. Meanwhile, the Liberals would say the public system should be limited to a safety net function, with the private system growing in size.
Two tier systems are also common in developing countries, where the government first established the underlying healthcare infrastructure, but as incomes have risen and urbanization has unfolded new private institutions have sprouted up.
As you can see, there are many ways a functional universal healthcare system can be achieved. Denmark, Taiwan, Switzerland, and Australia all have different systems, yet all of them are able to achieve universal access to quality care at an affordable cost to the public.
Despite this fact, these systems are not interchangeable. Each comes with pros and cons, and the appropriateness of any specific approach depends on the context.
I’ll be releasing a piece soon that explains my thoughts on this debate. For now, what are your thoughts? I’m curious to know! Leave your favorite approach and your case for it in the replies. I truly believe that this very critical part of the healthcare debate needs more attention.
People from all over the political spectrum need to know that there is a model of universal healthcare for them. From the market-oriented to the socialistic, there are many paths to the destination of universal healthcare. The question we should be asking ourselves is not whether we should pursue one of these paths but rather which one of these paths should we pursue.
I've always been ambiguous on what type of healthcare system to have since I never researched much into it. I suppose I just had other interests that made me more excited about, I think. I'll be looking forward to your other post.
I prefer two tiered system for the simple reason that while I don't want govt. to dominate our healthcare but from my personal experience I have seen people finding various options of private healthcare too complicating or sometimes not getting around to having a coverage at all due to various personal reasons. So I want an automatic universal fall back option for them aka public option.
Which of these system in general best promotes(or is less of a hinder in) innovation and research? Also which system(in general again ofc) is more adoptive to innovations?